


เฉลยโจทย์ NL2 เม.ย. 68 : AF with RVR ในผู้ป่วยหมดสติ
โจทย์:
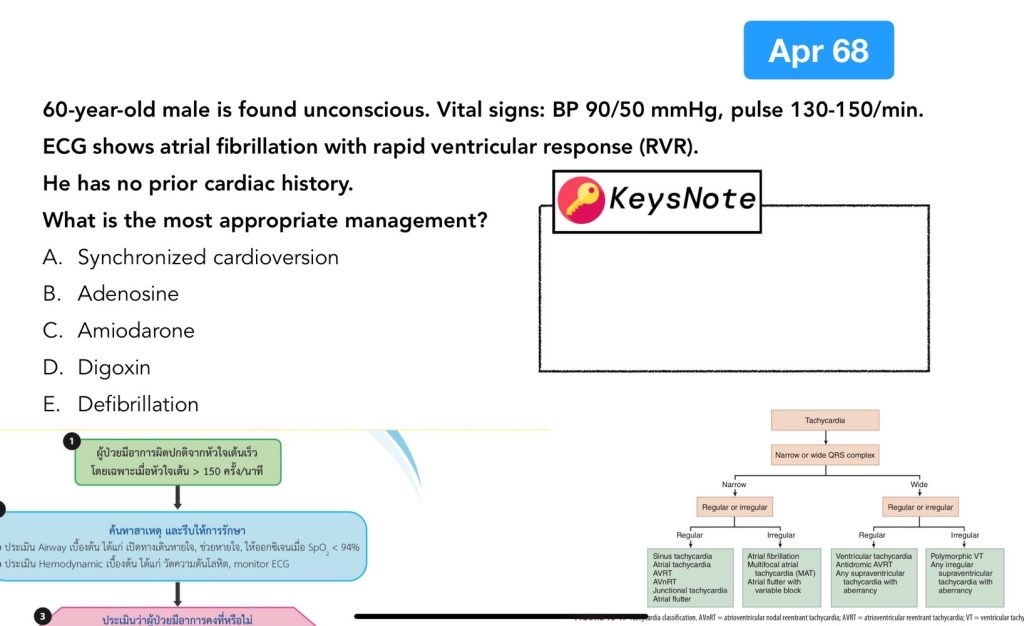
A 60-year-old male is found unconscious. Vital signs: BP 90/50 mmHg, pulse 130–150/min. ECG shows AF with RVR. He has no prior cardiac history. What is the most appropriate management?
ตัวเลือก:
A. Synchronized cardioversion
B. Adenosine
C. Amiodarone
D. Digoxin
E. Defibrillation
การวิเคราะห์โจทย์
- Point สำคัญ: ผู้ป่วยหมดสติ + ความดันต่ำ (BP 90/50 mmHg) + HR 130–150 irregular → เป็น hemodynamically unstable AF with RVR.
- ECG finding: atrial fibrillation (ไม่เห็น P wave, irregularly irregular QRS) + ventricular rate สูง.
- Guideline: ตาม ACLS “Unstable tachyarrhythmia → Immediate synchronized cardioversion.”
การวิเคราะห์ช้อยส์
A. Synchronized cardioversion → ถูกต้อง
เป็นการรักษาที่เหมาะสมที่สุดในผู้ป่วย AF with RVR ที่ unstable. ขนาดพลังงานที่แนะนำ: 100–200 J biphasic. ทำให้จังหวะหัวใจกลับสู่ sinus rhythm และ perfusion ดีขึ้น.
B. Adenosine → ไม่ถูกต้อง
ใช้ใน paroxysmal SVT (AVNRT/AVRT). ไม่ได้ผลกับ AF.
C. Amiodarone → ไม่เหมาะสม
ใช้ใน AF ที่ stable หรือต้องการ rhythm control. แต่ onset ไม่เร็วพอในผู้ป่วยหมดสติ.
D. Digoxin → ไม่เหมาะสม
ใช้ rate control ใน stable AF โดยเฉพาะ heart failure. แต่ onset ช้าเกินไป.
E. Defibrillation → ไม่ถูกต้อง
ใช้ใน VF/pulseless VT. ในโจทย์ยังมี pulse → ต้อง cardioversion.
เฉลย
คำตอบที่ถูกต้อง: A. Synchronized cardioversion
Discussion เพิ่มเติม
- Stable AF with RVR: ให้ยา rate control เช่น beta-blocker, diltiazem, digoxin หรือ amiodarone.
- Unstable AF with RVR: ต้อง cardioversion → ถ้าไม่สำเร็จอาจ repeat shock หรือให้ IV amiodarone.
- ข้อสอบ NL2 เม.ย. 68: จุดหลอกคือช้อยส์ Amiodarone/Digoxin → key คือ “unconscious, hypotension” → ต้อง cardioversion.
การจัดการตามแนวทาง Flowchart- Tachycardia Guideline
ในผู้ป่วย tachyarrhythmia (>150 ครั้ง/นาที) ต้องประเมิน Airway, Breathing, Circulation, oxygen saturation, ความดันโลหิต, monitor ECG.
ถ้ามีอาการ unstable (SBP < 90, shock, poor tissue perfusion, chest pain, acute heart failure) → Synchronized cardioversion ทันที.
ถ้า stable → แยกตาม QRS morphology:
- Regular narrow QRS: vagal maneuver → adenosine → β-blocker หรือ calcium channel blocker
- Irregular narrow QRS (AF with RVR): ให้ rate control (β-blocker, verapamil, diltiazem, digoxin หรือ amiodarone ถ้ามี HF)
- Regular wide QRS: ใช้ antiarrhythmic เช่น amiodarone หรือ cardioversion
- Irregular wide QRS: อาจเป็น AF with WPW → ห้าม AV nodal blocker, ใช้ amiodarone หรือ cardioversion
รายละเอียดเพิ่มเติมจากตำรา
Description
Atrial fibrillation (AF) เป็น narrow-complex tachycardia ที่พบบ่อย เกิดจาก multiple atrial foci ที่ firing พร้อมกัน → atrium quivering → ventricular filling ไม่ดี, cardiac output ลดลง. ECG hallmark: ไม่มี P wave, QRS irregularly irregular.
Clinical significance
สัมพันธ์กับ ischemic/valvular heart disease. สาเหตุอื่น ๆ เช่น cardiomyopathy, myocarditis, alcohol binge (“holiday heart”), thyrotoxicosis, blunt chest trauma. มักมี left atrial enlargement ใน chronic AF.
แนวทางการทำ Cardioversion
- Pharmacologic: ใช้ vernakalant, flecainide, propafenone (ถ้าไม่มี structural heart disease/ severe HF).
- IV Amiodarone: ใช้ใน AF + HF หรือ structural heart disease.
- Electrical cardioversion: แนะนำใน symptomatic หรือ persistent AF และใน unstable case.
- Pharmacologic cardioversion: ทำได้เฉพาะ stable AF และควรพิจารณา thromboembolic risk.
Amiodarone dosing
– Loading: 150 mg in 5% DW 100 mL IV drip over 30 min (~200 mL/hr).
– Maintenance: 900 mg in 5% DW 500 mL IV drip over 24 hr (~20.8 mL/hr).
Rate control drugs
- Diltiazem: 60–90 mg PO QID (immediate release). หลีกเลี่ยงใน HF with reduced EF.
- Metoprolol: 25–50 mg PO BID. ระวังใน asthma/COPD.
Treatment overview
การรักษา AF ใน ED มี 3 เป้าหมายหลัก: (1) Ventricular rate control (2) Rhythm conversion (3) Anticoagulation ป้องกัน arterial embolism.
การเลือกแนวทางขึ้นกับ stability, duration, และชนิด AF (paroxysmal, persistent, permanent). ใช้ CHA2DS2-VASc score เพื่อประเมิน risk. หากเป็น recent-onset AF with RVR + hypotension, ischemia, หรือ pulmonary edema → ต้อง urgent electrical cardioversion.
เทคนิคการติวสอบ NL2
- คำสำคัญ “unconscious, hypotension, shock, chest pain” → ตอบ cardioversion.
- Stable → ใช้ rate control drugs หรือ rhythm control.
- NL2 ชอบถามการแยก stable vs unstable arrhythmia.
Post-test: AF with RVR (NL2 เม.ย. 68)
1. ผู้ป่วย AF with RVR ที่มี BP 80/50 mmHg หมดสติ ควรทำอย่างไรเป็นอันดับแรก?
เฉลย: Synchronized cardioversion ทันที เนื่องจากเป็นภาวะ unstable tachyarrhythmia.
2. Digoxin ใช้ควบคุม ventricular rate ใน AF with RVR ได้เมื่อใด?
เฉลย: ใช้ในกรณีผู้ป่วย stable AF with RVR โดยเฉพาะถ้ามี heart failure แต่ไม่เหมาะกับผู้ป่วยที่ unstable.
3. ความแตกต่างของ Defibrillation และ Synchronized cardioversion คืออะไร?
เฉลย: Defibrillation ใช้ใน VF/pulseless VT โดยไม่ sync กับ QRS ส่วน Synchronized cardioversion ใช้ใน tachyarrhythmia with pulse เช่น AF with RVR ที่ unstable.
4. ยาที่นิยมใช้เป็น rate control ใน stable AF with RVR มีอะไรบ้าง?
เฉลย: β-blocker (metoprolol), Calcium channel blocker (diltiazem, verapamil), Digoxin (โดยเฉพาะถ้ามี HF), และ Amiodarone ในบางกรณี.
5. ในผู้ป่วย AF with RVR ที่สงสัย WPW syndrome ห้ามใช้ยากลุ่มใด?
เฉลย: ห้ามใช้ AV nodal blocker (เช่น digoxin, verapamil, diltiazem, β-blocker) เพราะอาจทำให้ conduction ผ่าน accessory pathway เพิ่มขึ้น → เสี่ยง VF. ควรใช้ Amiodarone หรือทำ cardioversion.